





 11 / 12
11 / 12

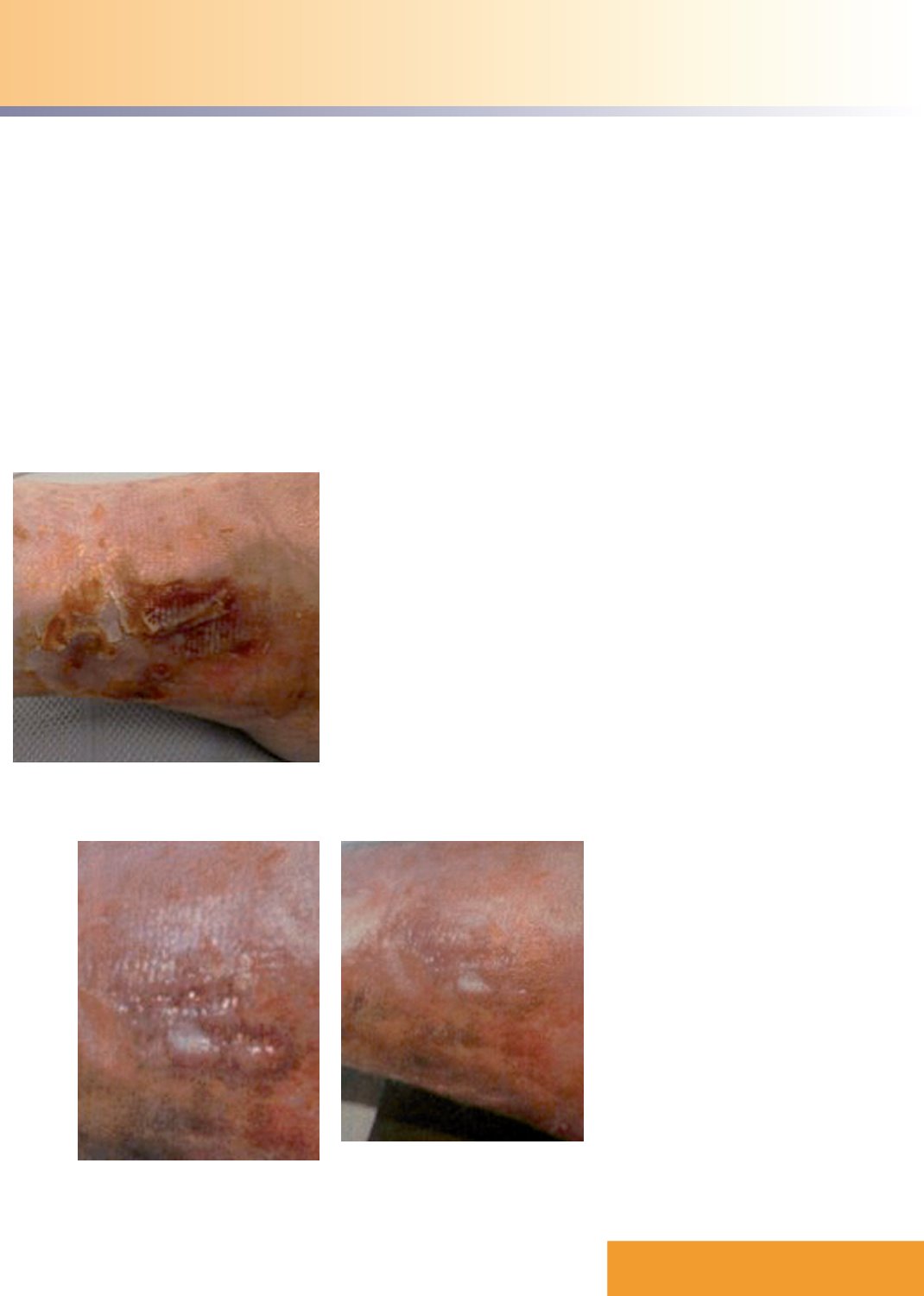
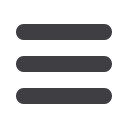
Figure 1.
Unhealed skin tear on the patient’s
lower shin.
Figure 2.
The wound reducing in size as treatment
with Actilite Protect progresses.
Figure 3.
The wound demonstrating growth
of granulation tissue and further
reduced size.
CASE REPORT 8
In this case, a trauma to
the shin resulted in a wound
that required exudate
management and an
antimicrobial dressing.
This patient was a 74-year-old
woman who was being cared for
in a nursing home. She had an
unhealed skin tear on her lower shin
caused by a trauma to the leg that
had occurred four weeks previously.
Before the evaluation it had been
treated with a foam dressing that
was changed every two days.
The patient had a poor
nutritional status but no underlying
medical conditions and she was a
non-smoker. Antibiotic s were not
used either before or during
the evaluation.
Wound progress
During the evaluation an Actilite
Protect dressing (10x10cm) was
used, as the foam can absorb
mild-to-moderate exudate and
the Manuka honey is a natural
antimicrobial, which can help with
debridement — both qualities that
the clinician thought might help
with this particular wound. The
dressing also has an atraumatic
silicone wound contact layer
designed for pain-free removal.
After two weeks of treatment the
clinician rated the product as ‘2’ on
a scale of 1–5 for ease of use, where
‘1’was ‘very easy’ and ‘5’was ‘very
difficult’— the dressing was also
found to be easy to apply and remove
(both rated ‘2’ on the five-point
scale). The dressing was considered
to be atraumatic to the wound bed
and the periwound skin (rated ‘4’
where a score of ‘5’was considered
‘atraumatic’), and it was reported to
have conformed well to the wound.
The dressing remained intact upon
removal and stayed in place as long
as had been expected, without the
edges rolling.
During the two-week evaluation
there had been no pain on application
or removal and there was no need for
analgesia during dressing changes. In
fact, no pain was reported throughout
the entire evaluation. When the
patient was asked about the new
dressing regimen, she rated it as very
comfortable and was satisfied with the
dressing’s performance (rating it‘2’
on a five-point scale where‘1’was
‘very satisfied’).
By the end of one week of
treatment the wound bed consisted
of 50% granulation tissue and by the
end of two weeks this had risen to
100%. The wound, which measured
10x5cm upon presentation and was
reported to have critical colonisation,
healed after being dressed with
Actilite Protect every three days.
The periwound skin did develop
signs of maceration during the
evaluation, and the clinician
commented that it would be
necessary to use barrier protection on
the periwound area.
The clinician was unable to say
whether the Manuka honey in the
dressing had treated any infection,
although she did state that the
product had positively contributed
to the wound’s healing. She was
particularly impressed by the fact that
Actilite Protect is a single dressing
that does not require a secondary
dressing, and felt that this made it
easier to apply.
The clinician did express some
concerns abo ut the shape of the
dressing and suggested that an oval
shape would prevent any rolling
of the edges when using it on
awkwardly positioned wounds (such
as on the buttocks).
JCN supplement
2015,Vol 29, No 4
11