








 5 / 24
5 / 24

JCN
Supplement 2016
5
and cleansing cloth which offers
atraumatic cleansing and debridement
of a wound and the surrounding skin,
without the use of water, any extra
surfactant or buckets (Downe, 2014).
It effectively prepares the wound
bed for healing by gently removing
barriers to healing such as slough,
debris and biofilms.
Dead and contaminated tissue
provide the perfect environment
for bacteria to grow, therefore their
removal reduces the risk of infection,
and facilitates accurate wound
assessment as the wound bed is more
easily visible.
UCS can be used on acute and
chronic wounds, postoperative
wounds, and wounds healing by
secondary intention, leg and diabetic
foot ulcers, peristomal skin, burns,
ports of entry for catheters, and
percutaneous endoscopic gastrostomy
(PEG)/ percutaneous endoscopic
jejunostomy (PEJ) tubes. It can be
used on all types of skin conditions,
including dry, hyperkeratotic skin (see
below), and is safe for use on fragile
skin and thus is suitable both for the
elderly and very young.
Active ingredients in UCS
Unlike other debridement pads
or cloths, the UCS cloth is pre-
moistened with active ingredients,
containing a surfactant, a mild
keratolytic and aloe vera.
Surfactants are cleansers that
penetrate the surface of a wound,
providing deep and effective
cleansing in just a few minutes. The
surfactants used in UCS are gentle,
non-allergenic cleansers which are
non-cytotoxic, and so cause no harm
to healthy tissue or cells.
The mild keratolytic helps
to soften any hardened skin on
the surface (horny layer of the
epidermis), allowing it to shed.
Typically in hyperkeratosis, the skin
is so dry and dehydrated that it
cannot naturally shed — leading to
a brown discoloured appearance to
the skin — and so removal of this
dehydrated layer requires rehydration.
The combined action of UCS cleans,
softens and allows better penetration
of the moisturiser, the final ingredient
in UCS —
aloe vera barbadensis
. This
provides a degree of moisture to
improve the skin’s integrity and has
anti-inflammatory and antimicrobial
properties (Rajeswari et al, 2012).
The UCS cloth is soft and pliable,
making it easy to get into those
difficult-to-reach places such as
between the toes, under skinfolds
(Downe, 2014), as well as cleaning
around the wound margins, which
is particularly important for cell
migration during epithelisation. The
cloth can also be cut, which allows
one cloth to be used safely for multiple
wounds, without the risk of cross-
contamination, and providing a safe
and more cost-effective treatment
option. The construction of the UCS
cloth also means that clinicians
have closer contact with the wound
bed while using the cloth, making
navigation more effective.
Accessing UCS on prescription
UCS can be found in the‘Physical
debridement’category of the drug
tariff. The debridement cloths are
available in boxes of 10 individually
packaged sterile pouches and are
simple for patients to use between
surgery appointments if appropriate.
UCS is the least expensive option
available in the physical debridement
category and the only pre-moistened
debridement cloth.
SUMMARY
In the author’s clinical experience,
providing holistic and optimal
patient care in a busy clinic can be
challenging. Allocated time slots are
short and patients are many and
varied. Effective management of
patients with wounds depends on
taking a systematic, holistic approach
to assessment. Focusing on the whole
of the patient and not just the‘hole’in
the patient is essential to ensure that
the underlying cause of the wound is
known (Hampton and Collins, 2004).
Using UCS for cleansing and
debriding is a quick, safe and cost-
effective alternative to washing legs in
buckets. It facilitates assessment and
healing, reduces time and risk of injury
to the nurse, while still offering the
patient the experience of having their
legs washed and cleaned.
To cite this article:
Gillies A (2016) Effective
debridement can be achieved in a busy
clinic environment.
J General Practice Nurs
2(2):
54–5
REFERENCES
Downe A (2014) How wound cleansing and
debriding aids management and healing.
J
Community Nurs
28(4):
33–7
Dowsett C, Newton H (2005) Wound bed
preparation: TIME in practice.
Wounds UK
1(1):
58–70
European Wound Management Association
(2013)
EWMA Document: Debridement.
An updated overview and clarification of
the principle role of debridement
. Available
online:
http://bit.ly/1L1uD2VHampton S, Collins F (2004) Holistic wound
assessment. In: Hampton S, Collins F,
eds.
Tissue Viabilit
y. Whurr Publications,
London: 40–75
Rajeswari R, Umadevi M, Sharmila C, et al
(2012) Aloe vera: the miracle plant. Its
medicinal and traditional uses in India.
J
Pharmacognosy Phytochem
1(4):
118
Vowden P,Vowden K (2011) Debridement
made easy.
Wounds UK
7(4)
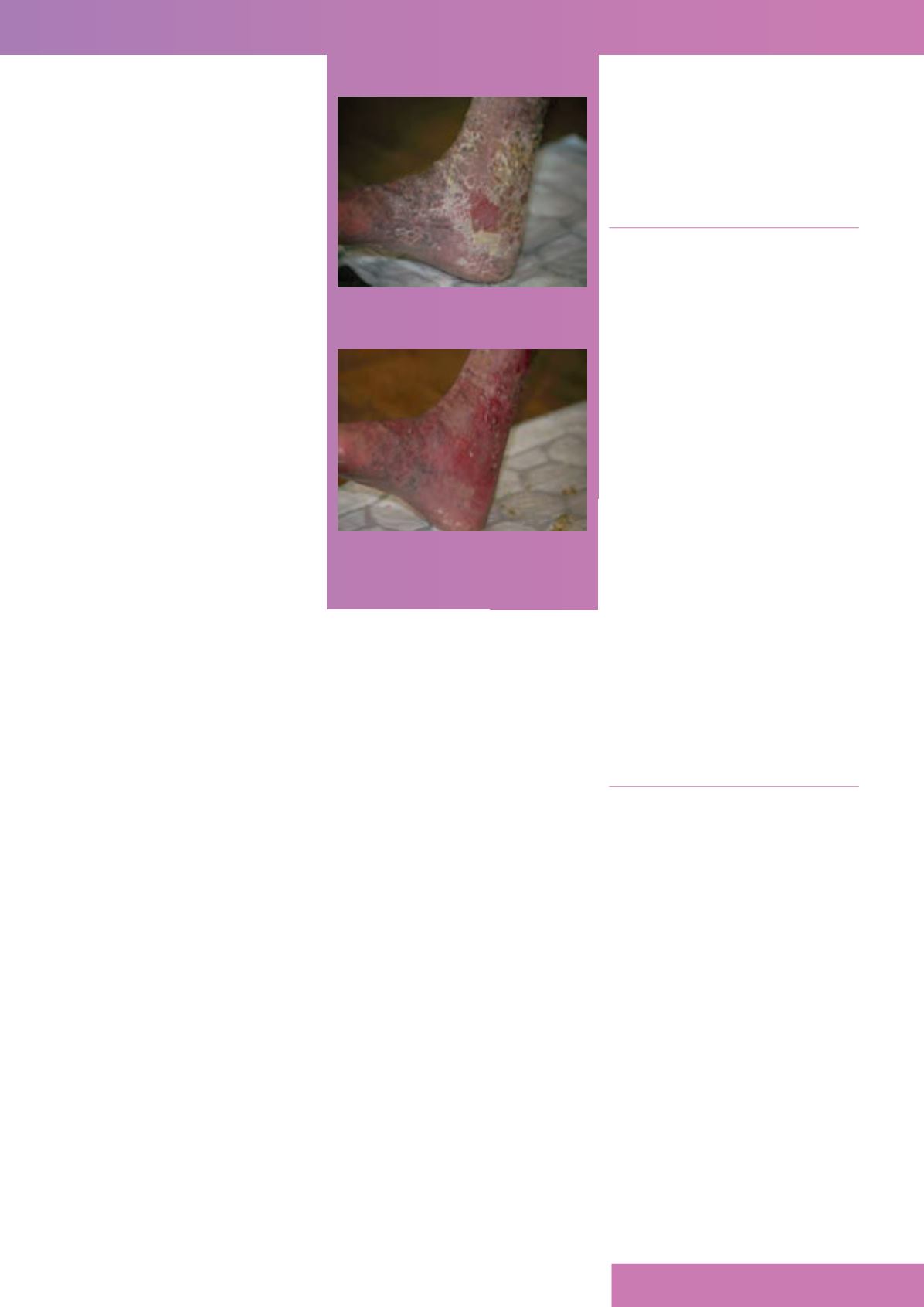
FIGURE 2.
After using UCS for less than
three minutes.
FIGURE 1.
Before using UCS.
JCN