








 11 / 24
11 / 24

JCN
Supplement 2016
11
DEBRIDEMENT
some wounds, others may need
intervention. Establishing a
good dermal bed is crucial to
wound healing.
Identifying and removing any
factors that will prevent or slow the
healing process such as damaged
and dead tissue, debris, and bacteria
is an important goal and will help
to minimise infection risk and
encourage healthy granulation
tissue to form, thereby aiding
healing.
The acronym TIME is a useful
tool that can be used to determine
objectives and plan appropriate
care. A summary of the four main
components is (Dowsett and
Newton, 2005):
`
T
issue management
`
Control of
I
nfection
and inflammation
`
M
oisture balance
`
Advancement of the epithelial
E
dge of the wound.
There are a number of
debridement techniques available
from surgical to physical/
mechanical methods (Foot in
Diabetes UK [FDUK] expert
working group, 2014), and
clinicians should be aware of
the options available.
It is not necessary for all
community nurses to be able to
perform all types of debridement,
however, they should have
sufficient understanding to
recognise which treatment is the
most appropriate for the individual
person and their wound (Vowden
and Vowden, 2011).
WOUND ASSESSMENT
The decision whether to debride a
patient’s wound must be based on a
comprehensive wound assessment
performed by a competent and
trained practitioner (Ousey and
Cook, 2012). The assessment must
be fully documented. Effective
debridement of the wound allows
the clinician to make a detailed
assessment of the wound bed and
surrounding area.
Traditional practice
The treatment of leg ulcers has
traditionally involved debridement
and cleansing with a bucket wash
or similar, often incorporating a
bath oil or emollient. This allows
the gentle removal of hyperkeratosis
and can be soothing for many
patients. However, some patients
such as those with diabetes-
associated neuropathy for example
may experience increased pain and
thus refuse this cleansing regimen.
This practice is also physically
demanding for the clinician or
healthcare assistant as each
bucket of water is likely to contain
approximately four litres of water
(weighing 4kg) and is therefore
heavy to carry from the tap to the
patient and back again. The whole
process of filling and moving
buckets of water is time-consuming
and physically demanding, in some
cases leading to musculoskeletal
issues for clinicians who have to
repeat the task regularly.
CLEANSING AND DEBRIDING
WITH A PRE-MOISTENED
CLOTH
UCS
™
(medi UK) is a premoistened
debridement device — the fluid
used to premoisten the cloth
helps to soften unwanted tissue in
preparation for gentle and effective
removal by the UCS cloth.
UCS is a class IIb medical device
and is therefore safe for use in
deep wounds where there may be
exposed tissue and bone etc. UCS
was approved for registration on
the Drug Tariff in England, Scotland
and Wales in May 2014.
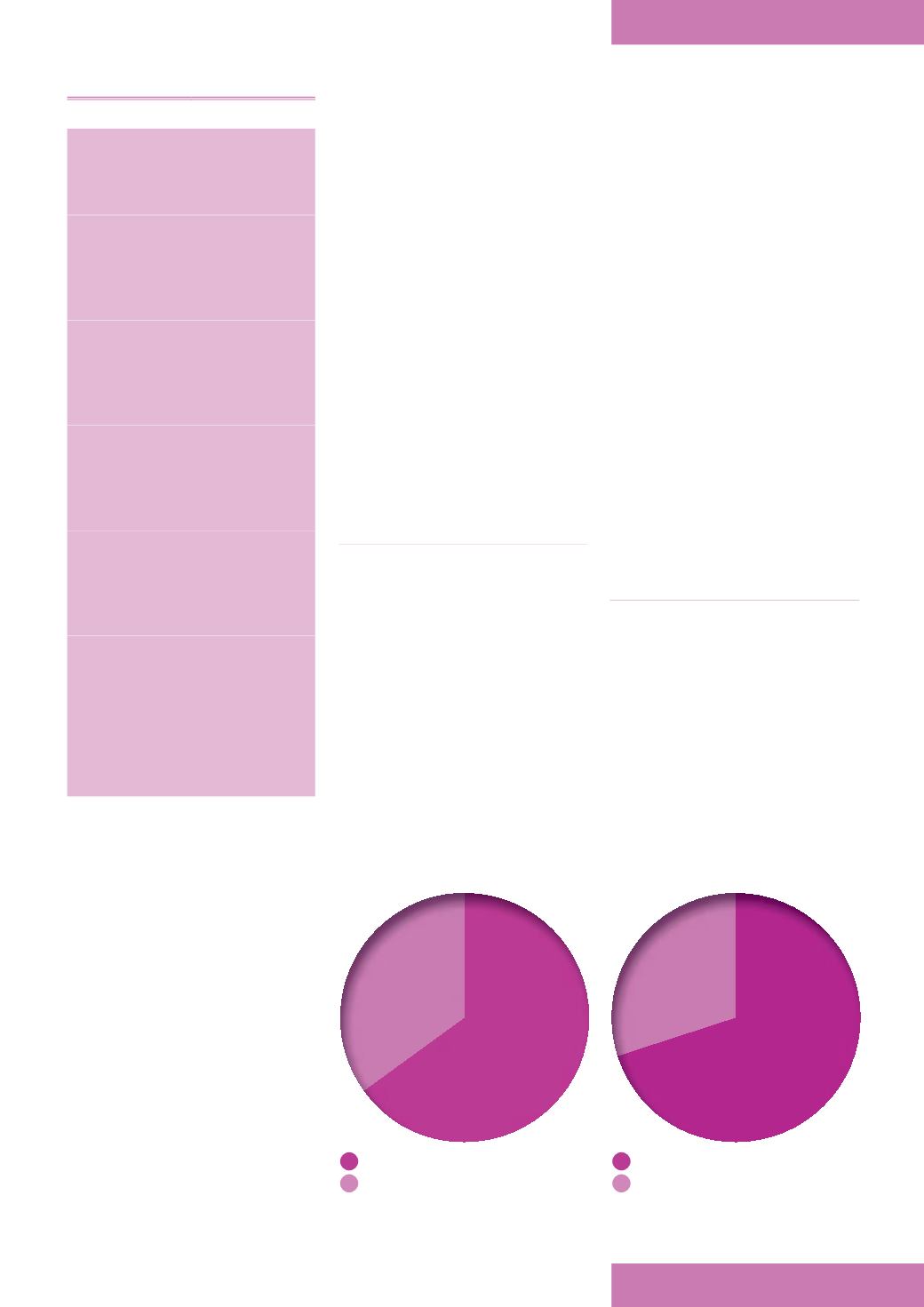
Figure 1.
UCS softness and durability.
Excellent
Good
Excellent
Good
Figure 2.
UCS ease of use.
KEY POINTS
In the community setting, leg
ulcer management involves both
care of the wound itself and the
skin of the lower limb.
Cleansing is vital to enure that
infection does not develop in
the wound itself and that the
integrity of the periwound skin
is maintained.
Maintaining the skin’s
barrier function is also vital,
as, without this, fluid loss,
inflammation, dryness and
infection can develop.
Wound exudate can also act
as an irritant to healthy skin,
particularly when permitted
to accumulate under
wound dressings.
Keeping the skin clean and
free of debris, alongside more
frequent dressing changes
can help in the treatment of
irritated skin.
This article highlights the use
of an innovative cleansing
product (UCS; medi UK), which
is designed as a pre-moistened
cloth that safely and efficiently
cleanses the wound of slough
and debris, while rehydrating
periwound skin.