
Date: 01 March 2021
The delivery of wound care in the current climate is challenging so effective solutions are more important than ever. It is vital that you are aware of the latest products and innovations that have the potential to improve outcomes.
Here, we present PolyMem®, a unique multifunctional polymeric membrane dressing that is indicated for a wide range of acute, chronic and specialist painful wounds.
Here, we present PolyMem®, a unique multifunctional polymeric membrane dressing that is indicated for a wide range of acute, chronic and specialist painful wounds.
Topics: Chronic wounds, Dressings, Wound care
Introduction
Dressing selection can be very challenging and confusing for healthcare professionals because of the sheer number of wound products available (Hampton, 2015). The use of an ‘all in one’ wound care dressing that can perform a number of functions across a range of different wound types can help to simplify dressing selection considerably (Denyer et al, 2015).PolyMem® is an ‘all in one’ dressing providing an ideal wound healing environment and less pain (Beitz, 2004 and Denyer et al, 2015).
PolyMem® dressings help to:
- Relieve pain (Beitz, 2004)
- Reduce oedema, bruising and the spread of inflammation into surrounding undamaged tissues (Beitz, 2004)
- Effectively manage and heal wounds
- Absorb exudate and provide a moist healing environment
How does PolyMem® work?
The dressings include a hydrophilic polyurethane matrix with a mild non-toxic wound cleanser (surfactant), a soothing moisturiser (glycerol), a superabsorbent and a semi-permeable film backing (not included in cavity products). The components work individually and synergistically to facilitate healing and relieve pain (Denyer et al, 2015).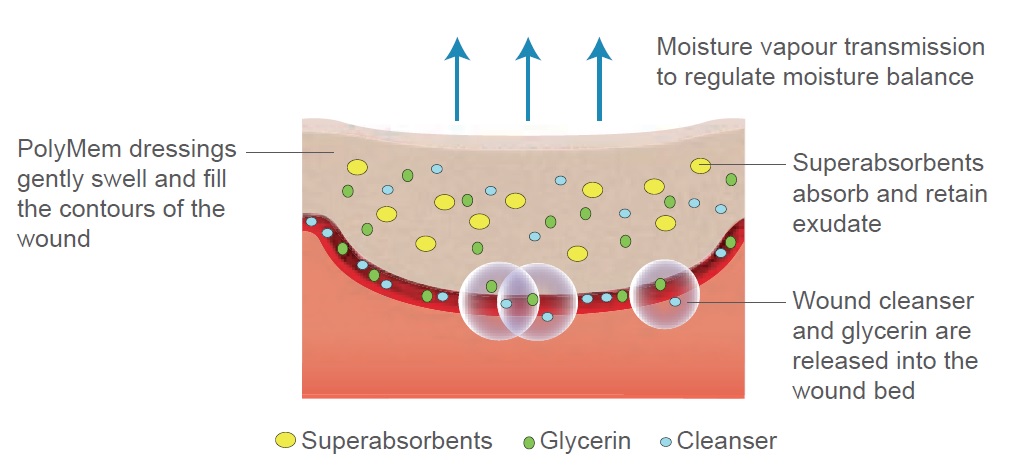 Figure 1. The structure and function of PolyMem®.
Figure 1. The structure and function of PolyMem®.PolyMem® is activated when it comes into contact with exudate to cleanse, absorb, fill and moisten the wound to promote healing. To activate the dressing components in dry, non-exuding wounds, e.g. necrotic wounds, moisten the dressing or wound slightly with saline or water prior to application.
Cleanses
When the dressing is applied, the surfactant cleanser is continually released into the wound where it breaks down the bond between devitalised and dead tissue and the wound bed, aiding autolytic debridement (Denyer et al, 2015).Moistens
The moisturiser (glycerol) is also simultaneously released helping to create a moist wound healing environment that supports debridement and healing, and also prevents the dressing from adhering to the wound bed (Denyer et al, 2015).Absorbs
Upon absorbing exudate, the dressing gently expands to fill the wound space and conforms to the surface of the wound, reducing the likelihood of leakage. Fluid is drawn from deep within the wound bed to ensure adequate hydration (Benskin, 2016). During the first few days of use, there is often a sudden increase in exudate as the dressing draws fluid from the wound and this indicates that the dressing is working.Fills
The superabsorbent particles bind wound exudate, holding it away from the wound bed and the peri-wound skin creating a moist environment while minimising the risk of maceration (Denyer et al, 2015).Inflammation
PolyMem® manages and contains the inflammatory response at the initial wound site and reduces inflammation in the surrounding tissues (Cutting and Gefen, 2019). This is achieved by altering the actions of certain nerve endings (nociceptors) and decreasing bruising, swelling and secondary injury.Pain
PolyMem® helps to inhibit the actions of some of the pain-sensing nerve fibres (nociceptors) which carry some of the pain messages after tissue-damaging injuries and inflammation.
PolyMem® Silver
PolyMem® Silver has small particles of elemental, metallic silver added and combines the features of PolyMem® with an added antimicrobial effect. The silver is retained within the dressing and is not released or deposited into the wound bed (Burd et al, 2007) which means the dressing can be used as frequently and for as long as desired.
Indications
PolyMem® is indicated for a wide range of acute, chronic and specialist painful wounds, including but not limited to:
- Acute wounds, e.g. abrasions, bruising, superficial and partial thickness burns and skin tears, surgical wounds and trauma wounds
- Chronic wounds, e.g. leg ulcers, pressure ulcers, diabetic foot ulcers and fungating wounds
- Specialist wounds, e.g. dermatological disorders (e.g. epidermolysis bullosa [EB]), graft and donor sites, exposed tendons and radiotherapy-induced skin damage.
PolyMem® Silver is indicated for malodorous and infected wounds from the above categories.
PolyMem® is not compatible with oxidising agents, such as hydrogen peroxide or hypochlorite solutions. It must also not be used, or it should be discontinued if patients show signs of sensitivity, irritation or allergy to the dressing or its materials. It should not come into contact with electrodes or conductive gels. Topical treatments are also not recommended in conjunction with PolyMem®.
WHICH POLYMEM® DRESSING?
PolyMem® is available in a range of sizes and presentations suitable for a range of uses (Table 1).Product presentation
Usage
PolyMem® adhesive or non-adhesive 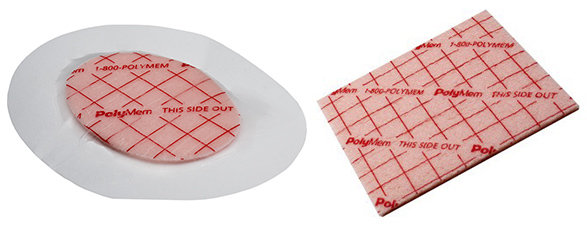
For dry to moderately exuding wounds
Silver adhesive or non-adhesive
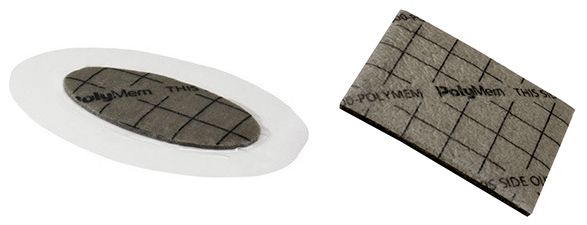
For infected and malodorous wounds
MAX

For greater absorbency and a longer wear time
Cavity wound filler (WIC)

In cavity wounds where the clinician has full visibility, PolyMem® WIC (both regular and silver) can be used
Finger/Toe
For finger and toe injuries
Roll
The dressing roll can be used on large wounds such as burn injuries, epidermolysis bullosa (EB) and radiotherapy-induced skin damage
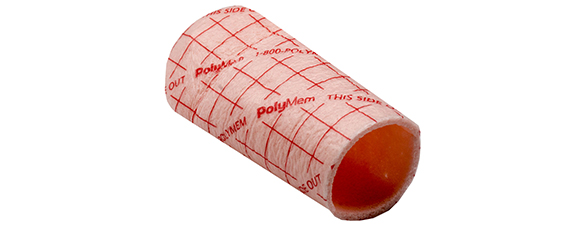
Tube dressing
The pre-cut tube dressing can be used for example in percutaneous endoscopic gastrostomy (PEG) tube sites and drainage tubes
Table 1. The different uses of each product presentation.
WHAT ARE THE BENEFITS OF USING POLYMEM®?
PolyMem® is designed to modulate and focus inflammation, relieve pain and facilitate healing:
Modulate inflammation
PolyMem® manages the inflammatory response in the wound and surrounding tissues (Beitz et al, 2004). The removal of excess fluid decreases the impact of oedema, reducing further potential damage associated with sustained cell deformation and tissue distortion, and prolonged obstruction of the vascular and lymphatic systems. It also alters the actions of certain nerve endings (nociceptors) (Beitz et al, 2004). The use of PolyMem® in clinical practice has shown reduced inflammation, oedema, bruising and pain (Kahn, 2000; Beitz et al, 2004; Cutting et al, 2015). Relieve pain
PolyMem® reduces the nociceptor response that normally leads to inflammation and pain without interfering with the normal inflammatory response required for wound healing to progress (Cutting et al, 2015). Due to the dressings cleansing and moisturising properties, PolyMem® is completely non-adherent and usually eliminates the need for wound bed cleansing during dressing changes (both known factors contributing to pain). This results in PolyMem® having an analgesic effect (Kahn, 2000; Beitz et al, 2004). Gefen (2018) found that PolyMem® may be useful for preventing pain in pressure ulcer ‘at risk’ sites, in vulnerable patients.Debride the wound
PolyMem® supports effective autolytic debridement by the surfactant reducing tension of necrotic tissue, whilst the combination of the components modulate and control the influx of critical inflammatory cells.Promote healing
Along with the benefits outlined above, wound fluid is drawn into the wound bed by PolyMem® ensuring adequate hydration and supporting a moist wound healing environment (Benskin, 2016).Simplify dressing selection
PolyMem® can be used on a wide variety of painful wounds, at different stages of would healing and has the potential to replace commonly used dressings such as polyurethane or silicone foams, hydrocolloids, hydrogels, alginates, and other traditional products.
What is the evidence for using PolyMem®?
Historical and current wound care practice focus’ on the management of tissue characteristics (De Leon et al, 2016) to optimise wound healing, and supportive pain control methodologies not directly associated with the dressings, other than non-adherent properties. A major point of differentiation within wound dressings is the use of PolyMem® to provide non-pharmacologic and non-narcotic analgesia.Controlled studies were performed by Kahn (2000) and Beitz et al (2004) in wound models to demonstrate the effect of PolyMem® on the response to mechanical and thermal stimuli and the preliminary evidence suggested that the dressing inhibits the activity of the nociceptive neurons in the epithelium which in turn blocks the response that generates swelling, inflammation and pain. Cutting et al (2015) provides a detailed review of acute and chronic wound inflammation and the role of PolyMem® with its supporting evidence. Cutting and Gefen (2019) provides an in-depth summary on how PolyMem® counters the effects of inflammation explaining the normal inflammatory response required for wound healing and abnormal inflammation in chronic wounds.
PolyMem® has been clinically indicated for use, frequently as first choice, in many of the different categories and types of EB in an International best practice guideline (Denyer et al, 2017). In a retrospective study evaluating six years’ experience using PolyMem® in EB, Denyer (2015) concluded that PolyMem® remains their dressing of choice as it was easy to apply and remove, reducing trauma and greatly reducing the duration of dressing changes. Healing rates were accelerated and the continual cleansing action by the surfactant helped to eliminate the need to cleanse the wound separately, minimising pain and trauma at dressing changes.
In a study of 40 patients at high risk of developing radiation-induced moist desquamation skin damage, Bode and Woodman (2008) concluded that the use of PolyMem® delayed the onset of acute skin reactions, demonstrated significant pain relief, reduced the risk of infection because of the constant cleansing effect, and acted as an anti-inflammatory. PolyMem® also received positive patient feedback and wound healing resumed quickly after the radiotherapy was discontinued.
Scott (2014) evaluated PolyMem® in 20 patients with head and neck cancer following radiotherapy. In diary entries, patients described the considerable pain relief and improved quality of life they experienced. Hegarty and Wong (2014) also demonstrated significant pain relief and increased healing rates in 23 patients whose skin reactions where managed using PolyMem® following radiotherapy.
Denyer et al (2015) highlights how a multifunctional wound dressing can impact positively on healthcare budgets that are under pressure. It also has a useful summary of published studies using PolyMem® in the clinical setting.
Edwards and Mason (2010) found in a case series of eight patients with ten infected burns that after using PolyMem® Silver, wound pain improved in all patients, there were low pain levels at dressing change, and low adherence to wound bed (completely atraumatic). Ease of application and conformability were rated highly and there was good wound exudate management. Benskin (2016) presents three case studies with infected wounds and outlined the goals of care were to resolve and prevent a return of infection, decrease pain, enable an immediate return to normal activities, and facilitate healing. In all 3 patients, the pain-relieving properties of PolyMem® Silver allowed resumption of activities within one day of initiating treatment, the dressings’ continuous wound cleansing ability kept the wounds clean and free of infection despite the challenging environment, and the wounds healed steadily. She concluded that managing infected acute wounds with PolyMem® Silver through to complete wound closure was time efficient for clinic staff and met all four patient goals of care. Benskin (2016) also provides an extensive literature search of clinical evaluations and reviews of PolyMem®.
Edwards and Mason (2010) found in a case series of eight patients with ten infected burns that after using PolyMem® Silver, wound pain improved in all patients, there were low pain levels at dressing change, and low adherence to wound bed (completely atraumatic). Ease of application and conformability were rated highly and there was good wound exudate management. Benskin (2016) presents three case studies with infected wounds and outlined the goals of care were to resolve and prevent a return of infection, decrease pain, enable an immediate return to normal activities, and facilitate healing. In all 3 patients, the pain-relieving properties of PolyMem® Silver allowed resumption of activities within one day of initiating treatment, the dressings’ continuous wound cleansing ability kept the wounds clean and free of infection despite the challenging environment, and the wounds healed steadily. She concluded that managing infected acute wounds with PolyMem® Silver through to complete wound closure was time efficient for clinic staff and met all four patient goals of care. Benskin (2016) also provides an extensive literature search of clinical evaluations and reviews of PolyMem®.
FOR MORE INFORMATION about PolyMem® visit,
Website: www.hrhealthcare.co.uk/portfolio/polymem
Watch Facebook Live: Understanding wound pain - the physiology of nociceptors and inflammation
Product enquiries: marketing@hrhealthcare.co.uk
Contact us: +44 (0)1482 631606
Watch Facebook Live: Understanding wound pain - the physiology of nociceptors and inflammation
Product enquiries: marketing@hrhealthcare.co.uk
Contact us: +44 (0)1482 631606
References
Beitz AJ, Newman A, Kahn AR et al (2004) A polymeric membrane dressing with antinociceptive properties: analysis with a rodent model of stab wound secondary hyperalgesia. J Pain 5(1): 38–47Benskin LL (2016) Polymeric membrane dressings for topical wound management of patients with infected wounds in a challenging environment: A protocol with 3 case examples. Ostomy Wound Manage 62(5): 42–50
Bode C, Woodman H (2008) Two novel treatments for the prevention and treatment of radiation induced moist desquamation. Poster presentation
Burd A, Kwok CH, Hung SC, et al (2007) A comparative study of the cytotoxicity of silver based dressings in monolayer cell, tissue explant, and animal models. Wound Repair Regen 15(1): 94-104
Cutting K, Gefen A (2019) PolyMem® and countering inflammation made easy. Wounds International. Available online: www.woundsinternational.com
Cutting KF, Vowden P, and Wiegand C (2015) Wound inflammation and the role of a multifunctional polymeric dressing. Wounds International 6(2): 41–6
De Leon J, Bohn GA, DiDomenico L, et al (2016) Wound care centers: Critical thinking and treatment strategies for wounds. WOUNDS 28(10): 3-24
Denyer J (2015) Six years’ experience of PolyMem® dressings used on children with epidermolysis bullosa (EB). Poster presentation. DEBRA International conference, 24 - 26 September. London, UK
Denyer J, Agathangelou C, White R, Ousey K, HariKrishna R (2015) PolyMem® made easy. Wounds International. Available online: www.woundsinternational.com/resources/details/polymem-dressings-made-easy
Denyer J, Pillay E, Clapham J (2017) Best practice guidelines for skin and wound care in epidermolysis bullosa. An International consensus. Wounds International. Available online: www.woundsinternational.com/uploads/resources/79912622fffa0956d1619feb123f35ed.pdf
Edwards J, Mason S (2010) An evaluation of the use of PolyMem® Silver in burn management. J Community Nurs 24(6): 16–19
Gefen A (2018) Managing inflammation by means of polymeric membrane dressings in pressure ulcer prevention. Wounds International 9(1): 250-256
Hampton S (2015) Selecting wound dressings for optimum healing. Nurs Times [online] 111(49/50): 20-23
Hegarty F, Wong M (2014) Polymeric membrane dressing for radiotherapy-induced skin reactions. Br J Nurs 23(Suppl20): S38-S46
Kahn AR (2000) A superficial cutaneous dressing inhibits inflammation and swelling in deep tissues. Pain Med 1(2): 187
Scott A (2014) Polymeric membrane dressing for radiotherapy-induced skin damage. Br J Nurs 23(10): S24-S30


