36
WOUND CARE TODAY
2015,Vol 2, No 1
FOCUS ON PRESSURE ULCERS
i
done by finding the cause of the
excessive exudate and the use of
appropriate dressings. For example,
infection or the rehydration of
necrotic tissue could increase the
level of exudate — the treatment
for necrotic tissue would be to
debride. This can be done in
several ways, including sharp and
surgical debridement or autolytic
debridement, or, as in the majority
of cases, the use of dressings
(autolytic debridement) (NICE,
2014). Some dressings such as
hydrofibres or hydrogels can be
used to aid autolytic debridement
(World Union of Wound Healing
Societies (WUWHS), 2007).
Dressings that absorb exudate
are available as primary and/or
secondary dressings. As a minimum,
any dressing selected should be
able to absorb and contain exudate
and enhance moist wound-healing
environment.
Dressing manufacturers usually
provide literature demonstrating the
amount of exudate that a dressing
will absorb and the recommended
wear time.
However, in the case of excessive
exudate it is not advisable to use a
dressing such as a hydrogel, which
will donate fluid to the wound
(WUWHS, 2007).
appropriate pressure-relieving
equipment.
Size
Measuring the size of the ulcer
and checking for any tunnelling or
undermining is important, not only
to chart the ulcer’s progress,
but also to select the correct
type and size of dressing.
To ensure that wound
measurement is consistent, the
patient should be in the same
position for each assessment
and the same method for
measuring the size and depth
of the wound should be used
(NPUAP/EPUAP/PPPIA,
2014). All assessments and
reassessments should be
recorded as per local policy.
Condition of surrounding skin
Checking the condition of the
surrounding skin is important
when seeking to choose the
correct dressing.
However, the condition of
the periwound skin can also be an
indication of the level of exudate
and the efficiency of the dressing
currently being used. For example,
a heavily exuding wound will cause
damage to the surrounding skin
— changing to a more absorbent
dressing and applying a barrier
product to the surrounding skin can
help with this.
Exudate
Wound exudate is an essential
component in the normal wound-
healing process. However, excessive
exudate can be a major challenge
for clinicians and a source of
embarrassment and discomfort for
the patient.
The aim is to provide a wound-
healing environment that maintains
the optimal amount of exudate to
promote healing. This is can be
Infection
In the case of infection, debridement
may also be required and where
appropriate an antimicrobial
dressing may address this. Some
antimicrobial dressings also have
autolytic properties which can
aid debridement and address the
wound infection simultaneously.
Antimicrobial dressings should
always be used in accordance with
local policies (Jones, 2014).
FURTHER MANAGEMENT
Pressure-relieving
equipment and
repositioning
If a patient with a pressure
ulcer is already being
managed on pressure-
relieving equipment such as a
pressure-relieving mattresses,
cushions, or chairs with
integral cushions, these will
need to be reviewed as will any
repositioning schedule.
If the equipment is not
effective it may need to be
changed, for example from a
high-specification mattress
to a dynamic mattress. This is
especially important where the
patient has a category three
or four ulcer (NICE, 2014;
NPUAP/EPUAP/PPPIA, 2014).
In order to aid healing of the
ulcer and prevent deterioration, it
is important to be able to identify
the underlying cause of the ulcer
and, where possible, treat this. For
example, if a patient with a pressure
ulcer on his or her sacrum has
limited mobility and sits in a chair all
day, it is probable that the cause of
the ulcer is the lack of mobility plus
the amount of time spent sitting.
In this case, management
would include pressure-relieving
equipment, a repositioning schedule
and, depending on the category of
Top tip:
Never leave slings or
manual-handling equipment
underneath a patient.
Top tip:
Provide supplements to patients
with pressure ulcers who are
QXWULWLRQDOO\ GHÀFLHQW
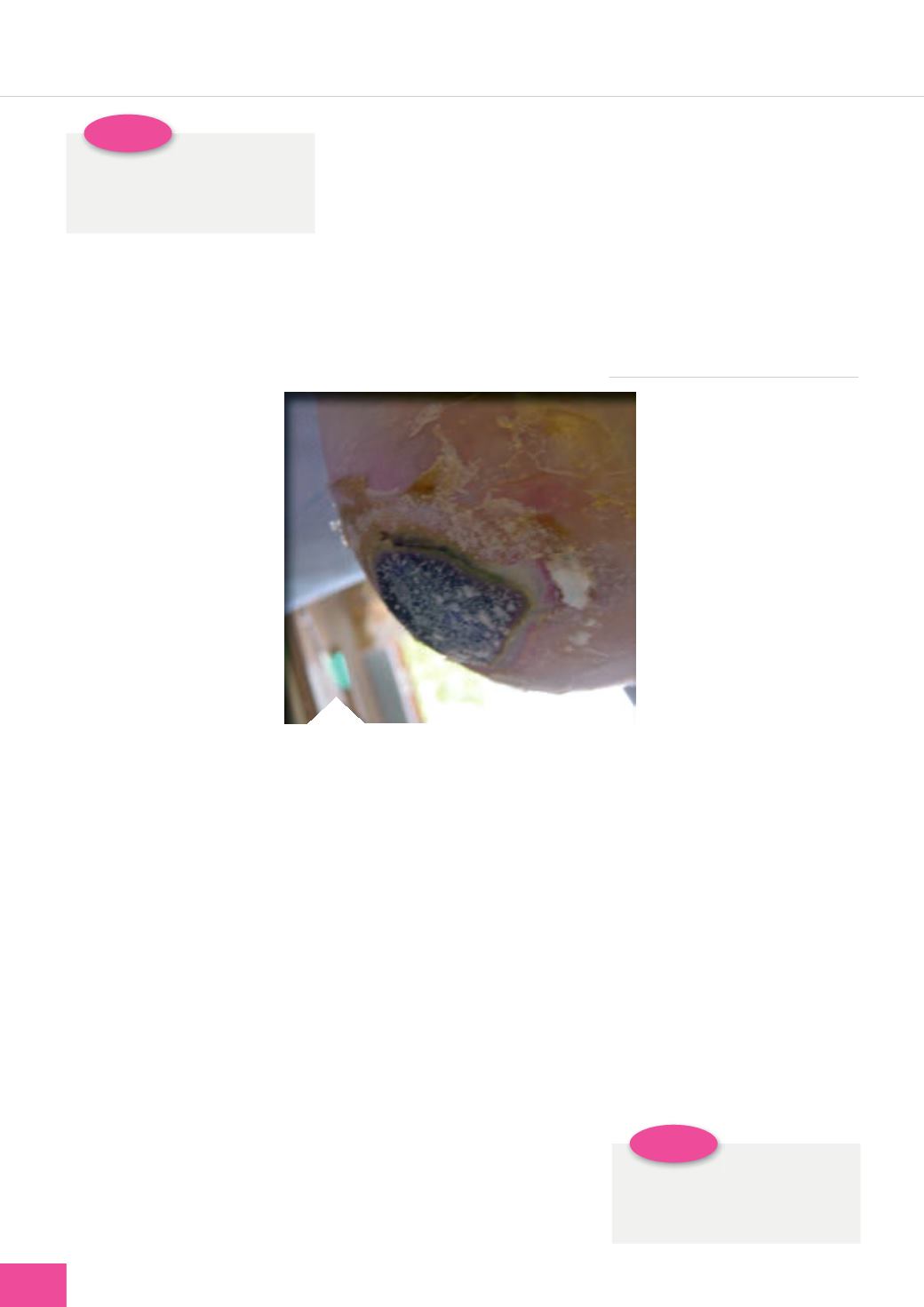
Figure 4.
A heel pressure ulcer demonstrating
significant eschar.


