Granulox
®
haemoglobin spray
This 85-year-old male patient
had a history of type 2 diabetes
going back for over 30 years. His
assessment also revealed that he
smoked 10–15 cigarettes per day
and drank alcohol (whisky) on a
daily basis.
The author found that he had an
ischaemic wound to the apex of the
second toe on his right foot
(
Figure 1
), which had been in place
for over 12 months (before the team
decided to begin treatment with
Granulox
®
[infirst Healthcare]).
Previous treatments included silver-
containing dressings (Aquacel
®
Ag; ConvaTec) and dressings that
incorporated honey (Medihoney
®
;
Dermasciences), as well as various
foam dressings.
At one of the twice-weekly
debridement sessions the author
noted a pocket of yellow pus
trapped around the bone at the
wound’s base, although there
was no necrosis in the wound.
There was also no pulse below
the patient’s knee. Despite this,
the surgeons were unwilling to
perform a bypass operation to re-
route bloodflow to the area mainly
because they felt that — due to his
age and smoking history — the
patient might not survive the three-
and-a-half-hour operation.
As mentioned above, the patient
was being reviewed twice-weekly
to debride the area and release
the build up of pus in the wound.
At these visits, the wound was
debrided, cleansed, photographed
and redressed. Due to his diabetes
and ischaemia, it was felt that
leaving the wound for any longer
than a few days at a time might
mean that an infection could
develop and spread undetected.
Starting on Granulox
®
Initially, the team began treating
the patient with Granulox twice-
weekly from 13 March, 2014.
Granulox was chosen due to a lack
of healing progress when using
various other product, as well as
the unwillingness of the surgeons
to operate. The author felt that
Granulox’s ability to provide oxygen
to the wound bed might prove
crucial to healing.
On 27 June, 2014 the bone at the
base of the wound was removed
with a scalpel and sterile forceps
(
Figure 2
). It had become loose and
the team felt that removing it would
give the wound a better chance
of healing.
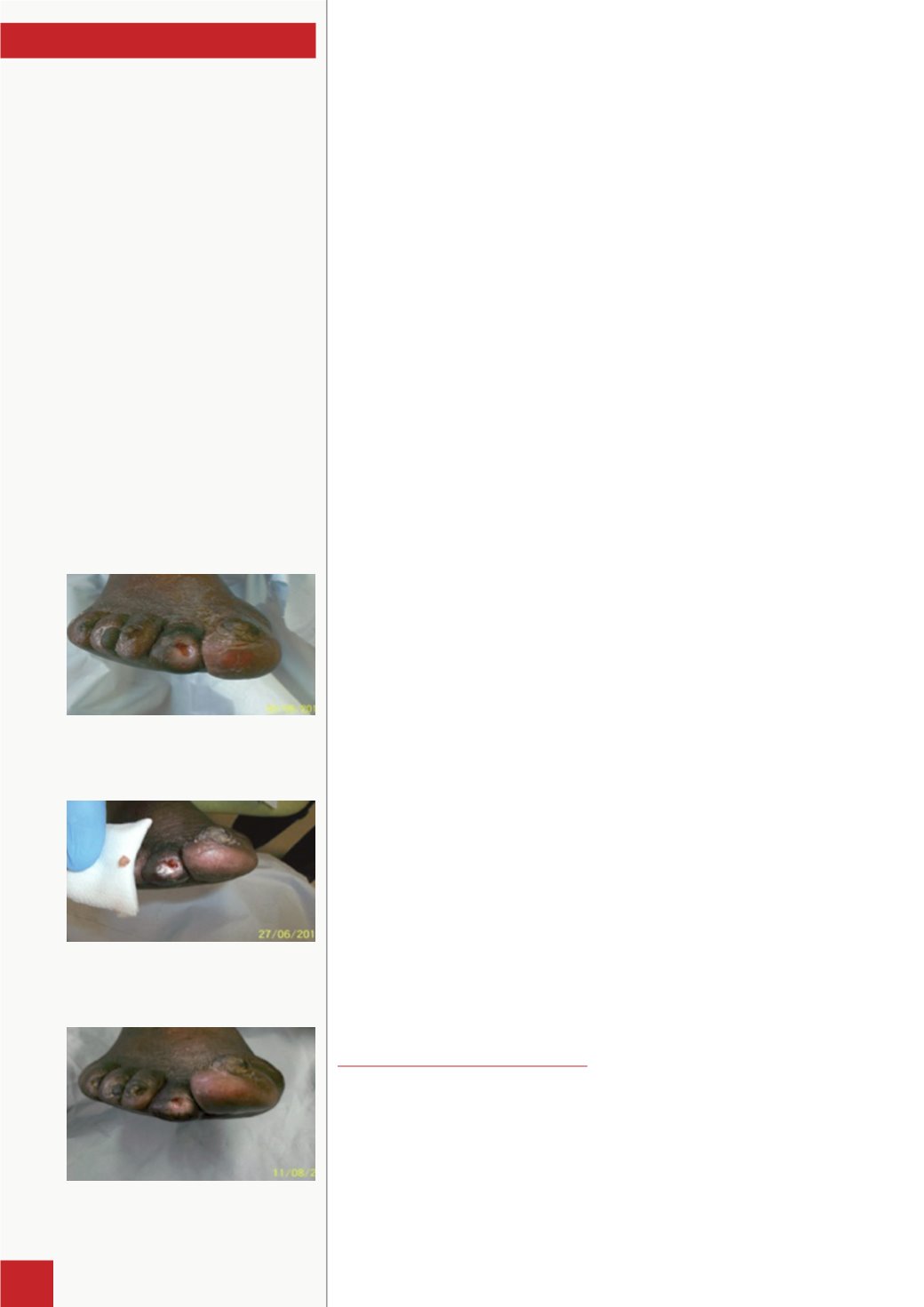
By 11 August, 2014 this patient
had received 41 applications
of Granulox. It was decided to
continue treatment as substantial
improvement had been noticed,
including decreased wound size
and reduced pain (
Figure 3
). For
example, on 13 March, 2014 the
wound measured 4x5cm, whereas
on 11 August, 2014 it measured
2x2cm — an 80% reduction. The
patient’s pain level also significantly
reduced from ‘7’ to ‘4’ on a verbal
pain scale of 1–10 (where ‘10’ was
the worst pain imaginable).
Finally, at a visit on 13 October
2014, the wound appeared
to be completely healed and
remains so at the time of writing.
Unfortunately, the patient has
developed another wound on the
little toe of his left foot, which
is currently being treated with
Granulox and Activheal
®
Foam
(Advanced Medical Solutions).
Case report
1
Figure 2.
On 27 June, 2014 — a fragment of bone
removed from the wound.
Figure 3.
On 11 August, 2014 — there has been a
decrease in wound width and depth.
Figure 1.
The wound on 2 May, 2014 after
debridement of the wound base.
2
This case shows how the introduction
of Granulox into the treatment regimen
of a longstanding ischaemic wound
in a patient who had diabetes and an
unhealthy lifestyle managed to put the
wound on a healing trajectory.


