68
SKIN CARE TODAY
2015,Vol 1, No 1
Table 1:
7RSLFDO WUHDWPHQWV IRU WKH ERG\
6WHS
$SSOLFDWLRQ
6LGH HIIHFWV UHVWULFWLRQV
Vitamin D analogues
(e.g. calcipotriol)
Twice a day, unless used
with topical steroids,
then once a day
i
Can sting especially on normal skin (generally
avoid face and flexures except calcitriol)
i
No more than 120g per week
i
Avoid if patient has compromised calcium levels
Topical steroid
(usually potent)
Once a day in conjunction
with topical vitamin D
analogue
i
Possible rebound of the psoriasis
on withdrawal
Combined steroid and
vitamin D
(i.e. Dovobet
®
, Leo)
Once a day
i
Has to be reviewed at four weeks
Dithranol (e.g.
Dithrocream™,
Dermal)
(infrequently used)
Once a day to well-defined
plaques only
Can be used short contact,
applied, left for increasing
amounts of time and then
washed off
i
Time-consuming to apply
i
Stains skin (and anything else that it comes
into contact with)
i
Makes normal skin sore
Tar (e.g. Exorex
®
, Forest
Laboratories)
(infrequently used)
Twice a day
i
Distinctive smell
i
Only weak concentrations available in
the community
* Always check current
British National Formulary (BNF)
for specific prescibing instructions
emollients can help to reduce itching
and scaling and are useful adjuvants
to other active topical therapies, such
as vitamin D analogues and topical
steroids (
Table 1
).
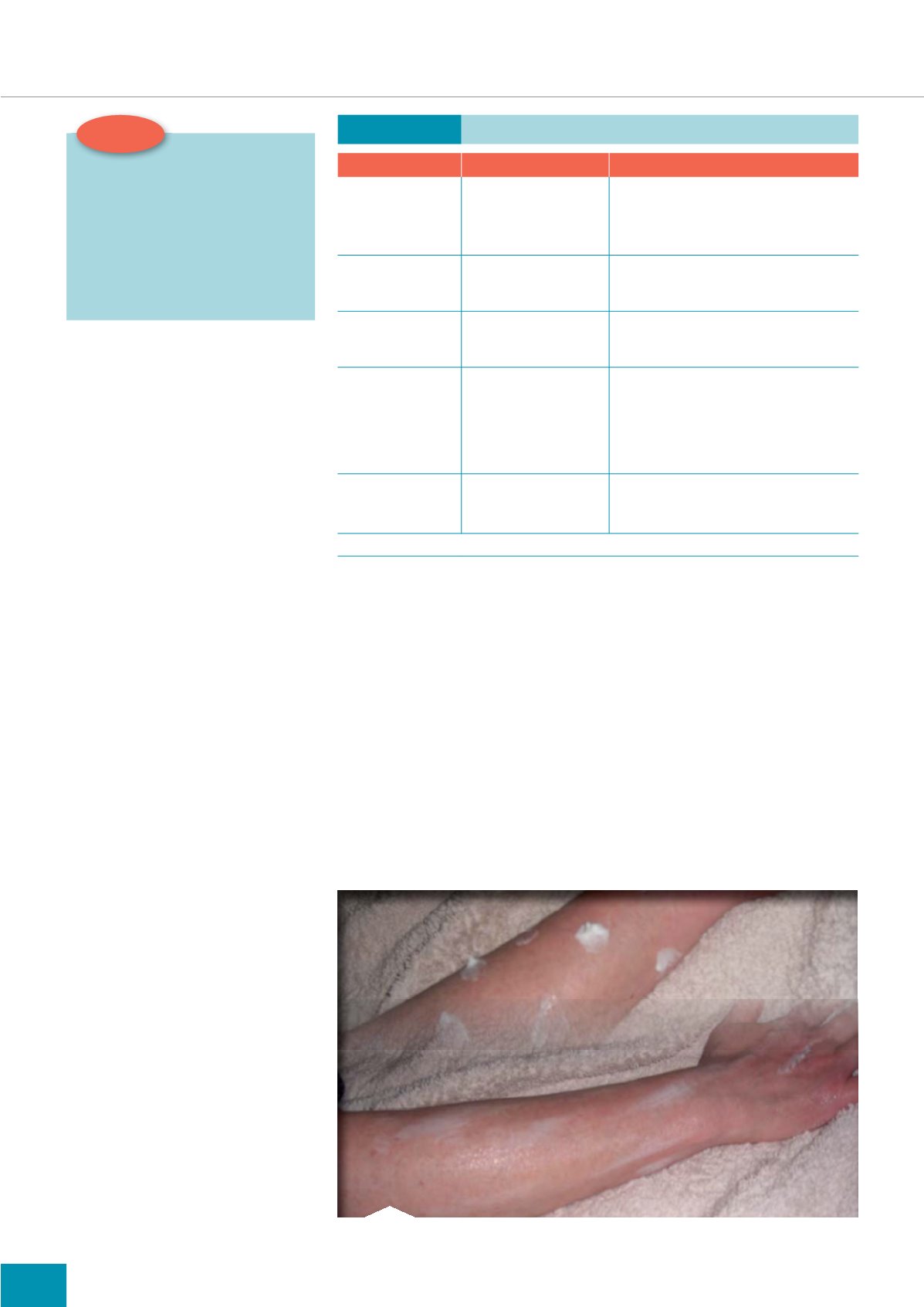
In terms of quantities to put on at
each application, there is no specific
quantity stated, however it needs to
be sufficient to cover the area and
leave a slight sheen (
Figure 2
).
Prescribed topical treatments
In addition to using emollients,
other topical therapies such as
those listed in
Table 1
should be
prescribed to reduce/control active
lesions.Vitamin D analogues, often
in conjunction with topical steroids,
are the first-line of treatment.
NICE (2012) lists tar along with
potent topical steroids alone as
second-line therapy and dithranol
as third-line therapy. The authors of
this article feel that the combined
product of topical calcipotriol and
betamethasone together (Dovobet
®
,
Leo) should be offered over the two
treatments separately, although
this does not comply with NICE
guidance. The combined therapy
offers a once-a-day treatment, which
is cheaper as only one prescription
item is needed.
Whichever treatment is selected,
careful patient education must be
undertaken so that expectations
are realistic. Treatments will often
show little sign of working until they
have been used consistently for 2–4
weeks. This can be very dispiriting for
patients, so they will need support.
When plaques start to resolve
they will not necessarily reduce
in size, but instead clear from the
middle outwards leaving a ring of
psoriasis with a flat middle. The
Top tip:
8VLQJ WKH ¶UXOH RI V· LV D KHOSIXO
ZD\ WR HVWLPDWH ERG\ VXUIDFH
DUHDV DIIHFWHG E\ SVRULDVLV 7KLV
LV EDVHG RQ WKH SULQFLSOH WKDW WKH
SDOP LV HTXDO WR DSSUR[LPDWHO\
RI WRWDO ERG\ VXUIDFH DUHD
5HPHPEHU H[SHULHQFH LV QHHGHG
WR FDUU\ RXW WKLV WHFKQLTXH
plaque has cleared completely when
the surface is smooth, i.e. there is no
bump when running a finger over it.
Some post-inflammatory marks, that
look almost like a bruise, may be left
on the skin even after treatment is
successful. These will take a month
or so to fade completely. If treatment
is continued after the plaque has
cleared, the skin is likely to become
red and sore.
Topical treatments for the scalp
Application of treatments to the
scalp is made more difficult due to
hair. NICE guidance recommends
Figure 2.
Applying emollients to the arm.
a four-week course of a potent
topical steroid (i.e. Betnovate scalp
application) as a first-line treatment.
This is effective if there are no
thickened plaques. However, if there
are thick, scaly plaques, the adherent
scale needs to be removed first for
subsequent treatments to be effective.
A combination ointment containing
coconut oil, salicylic acid and coal
tar rubbed into the scalp at night
and washed off in the morning is,
in the authors’ clinical experience,
the best way to do this. To apply
effectively the hair needs to be parted
in sections and treatment rubbed into
FOCUS ON PSORIASIS
i


