SKIN CARE TODAY
2015,Vol 1, No 1
17
factors such as religion, culture and
upbringing before beginning the
physical examination (Lawton, 2005).
Lesions should be measured
accurately and described and
documented on a body plan. This
description should include the
distribution, type, size, shape and
colour of the lesions. The surface
characteristics and texture (superficial
or deep) should also be recorded,
considering character, shape and
distribution (Fitzpatrick et al, 2001;
Lawton, 2005).
Character:
i
Is there redness (erythema),
scaling, crusting, exudate?
i
Are there excoriations, blisters,
erosions, pustules, papules?
i
Are the lesions all the same
(monomorphic), e.g. drug rash,
or variable (polymorphic),
e.g. chickenpox?
Shape:
i
Are the lesions small, large,
annular (ring-shaped), linear,
serpiginous (snakelike)
umbilicated?
i
Arrangement of multiple lesions:
grouped or disseminated,
scattered, discrete lesions
or diffuse?
Distribution:
i
Extent: isolated single lesion,
localised, regional, generalised
i
Is it acral (hands, feet), extremities
of ears and nose, in light exposed
areas or mainly confined to
the trunk?
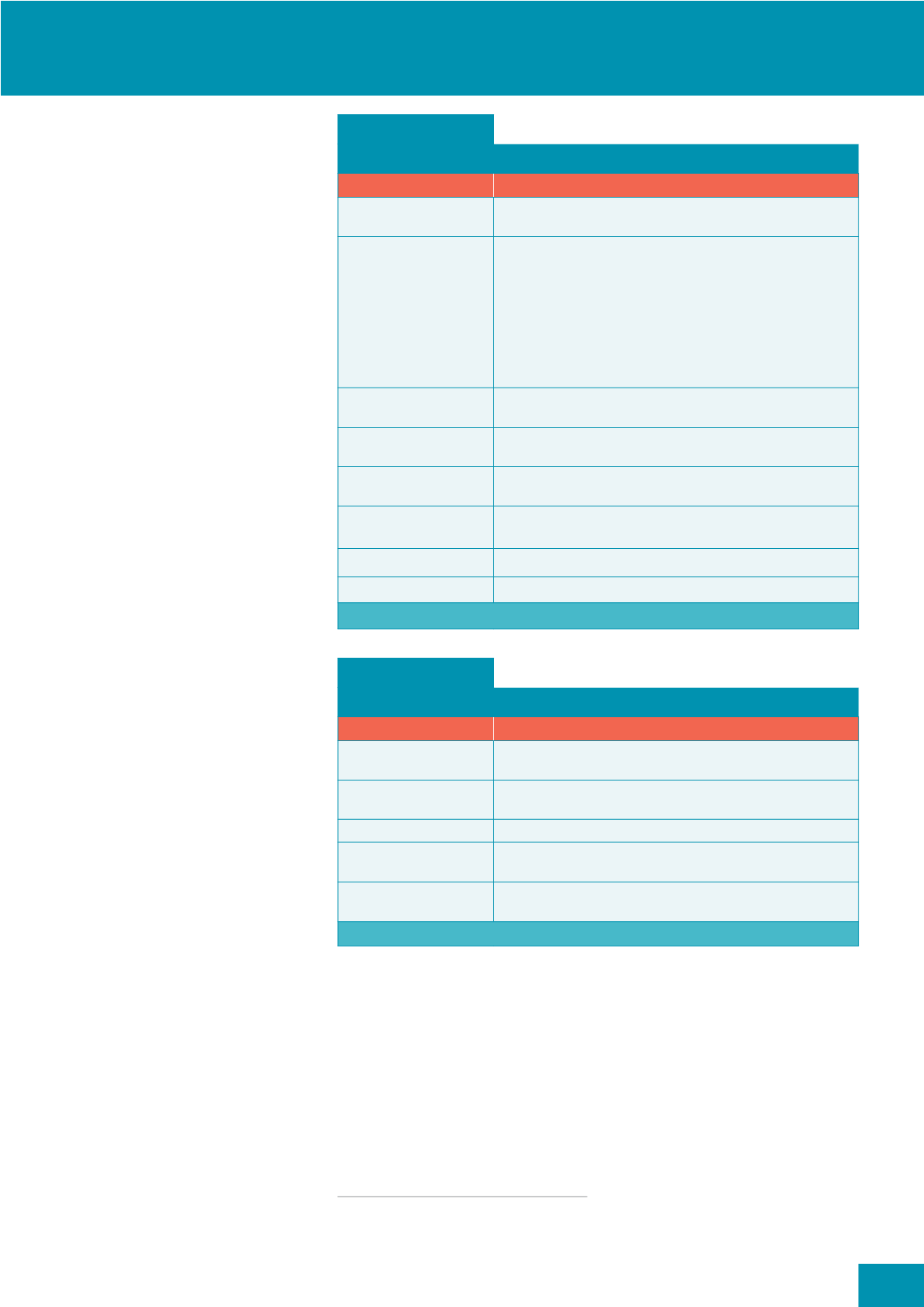
Lesions are classified as primary
(
Box 1
), which present at the initial
onset of the disease, and secondary
(
Box 2
), which are the result of
changes over time caused by
disease progression, manipulation
(scratching, rubbing, picking), or
from treatments applied to the skin
(Lawton, 2005).
Other factors to consider when
performing a physical assessment of
the skin is the range of skin colours
and hair types, as lesions which in
white skin appear red or brown,
appear black or purple in pigmented
skin, with mild redness (erythema)
Box 1:
Primary lesions
7\SH
'HVFULSWLRQ
Macule (e.g. Mongolian
blue spot)
A flat mark, a circumscribed area of colour change, brown, red, white, blue
or tan with smooth surface
Papule (e.g. scabies)
An elevated spot, palpable, firm, circumscribed lesion, generally less than
5mm in diameter. May be solitary or multiple and can be:
z
Acuminate (pointed), dome-shaped (rounded)
z
Filiform (thread-like), flat-topped, oval or round
z
Pedunculated (with a stalk)
z
Sessile (without a stalk)
z
Umbilicated (with a central depression)
z
Verrucous (warty)
Nodule
(e.g. rheumatoid nodule)
Elevated, firm, circumscribed, palpable, large solid lesion greater than
5mm in diameter — can involve all layers of the skin
Plaque (e.g. psoriasis)
An elevated, flat-topped, firm, rough, superficial papule greater than 2cm
in diameter, with well-defined or ill-defined borders
Wheal
An elevated, solid, transient, changing and irregular-shaped area of
cutaneous oedema.Variable in diameter, pale pink or white
Vesicle
An elevated, circumscribed, superficial fluid-filled blister less than 5mm in
diameter. They may be grouped
Bulla
A vesicle (blister) greater than 5mm in diameter
Pustule
A vesicle filled with pus
(Lawton, 2005; DermNetNZ, 2014a)
Box 2:
Secondary lesions
7\SH
'HVFULSWLRQ
Scale (e.g. psoriasis)
Heaped-up keratinised cells, flaky exfoliation, irregular, thick or thin, dry
or oily, variable size, silver, white or tan in colour
Crust (e.g. impetigo)
Dried serum, blood or purulent exudate, slightly elevated and
variable in size
Excoriation (e.g. atopic eczema)
Loss of epidermis, linear area usually due to scratching
Lichenification
(e.g. chronic eczema)
Rough, thickened epidermis; accentuated skin markings caused by
rubbing or scratching
Maceration
(skin surrounding leg ulcer)
Softened, soggy epidermis
(Lawton, 2005; PCDS, 2014a)
often being missed. Skin inflammation
commonly leads to post inflammatory
pigmentary changes — lighter (post-
inflammatory hypo-pigmentation)
and darker (post-inflammatory
hyper-pigmentation), which can
persist for a long time after the initial
inflammation and is often of great
concern to patients who think their
skin is permanently scarred.
ADDITIONAL DIAGNOSTICS
As part of assessment and diagnosis,
further tests may be required (PCDS,
2014a; DermNetNZ, 2014b). These
may include:
i
Diagnostic biopsies
: histological
examination for diagnosis and
immunofluorescence (IMF), which
looks at immune complexes in
many of the blistering conditions
i
Microbiological samples
of
scales, crusts, exudate and tissue
(including hair and nails) for
microscopy and culture, looking
for yeasts, fungi, bacteria, viruses
and parasites
i
Blood sampling
for diagnosing
and monitoring drug therapies
SKIN ASSESSMENT SKILLS
i


